Diagnosis
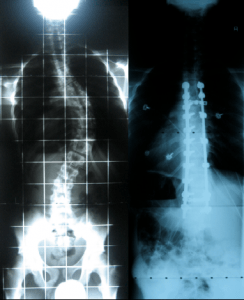
Dr. Stieber’s assessment includes a medical history, physical and neurological exam, and diagnostic testing with x-rays and other methods. The medical history may include questions about the parent’s genealogy and whether other family members have scoliosis. Dr. Stieber will check for underlying medical conditions that might otherwise be causing scoliosis. Additionally, the patient’s age, the onset of puberty, and growth history will help us determine the number of years that remain before the child reaches skeletal maturity. At skeletal maturity, curve progression may stop as long as the curve is less than 40-45 degrees. The curve may continue to progress throughout adulthood if the curve exceeds 40-45 degrees.